Promoting Local Health Traditions and Local Food Baskets: A Case Study from a Biocultural Hotspot of India(SITR7-9)
14.03.2023
SUBMITTING ORGANIZATION
M. S. Swaminathan Research Foundation, Meppadi, Kerala, India
DATE OF PUBLICATION
06/2022
REGION
Asia
COUNTRY
India
KEYWORDS
Biodiversity · Local health and food traditions · Self-help groups · Primary healthcare training · Home nutrition gardens · Immunity
AUTHOR(S)
N. Anil Kumar, V. V. Sivan, and P. Vipindas
LINK
Abstract
Degradation of socio-ecological production landscapes (SEPLs) triggered mainly by the impoverishment of biodiversity and the increasing incidence of climate catastrophes significantly challenges human health and food and nutritional security. Critical concern needs to be placed on ensuring both human and ecosystem health and contributing to nutrition-sensitive local food production and protection of SEPLs. As case points, we describe herein a few interventions and their impacts in promoting the conservation, cultivation, consumption, and commercial aspects regarding the medicinal and food plant diversity of a biocultural diversity hotspot in the Malabar region of India. The local communities of this region have historically possessed a wide array of local health traditions (LHTs) and local food baskets (LFBs) based on a landscape approach. Yet, this richness is being eroded or oversimplified, and as a result, many plants important for their local food and health value are becoming rare. The need for revitalisation of the LHTs and LFBs through homestead and landscape-level interventions is discussed in view of human immunity to infectious diseases. Recommendations are also suggested to address some of the policy gaps in promoting the sustainable management of SEPLs.
1 Context
Biodiversity is the major link between environment, food, medicine, and human health. Although areas rich in biodiversity have a correspondingly high number of potential pathogens that can impact human health negatively, these viruses often live safely in animal reservoirs. The services of ecosystems that are rich in biodiversity often have the capacity to shield as a protective factor to prevent transmission of infectious diseases (Romanelli et al., 2015). The research and communication needs, however, remain enormous for our modern society to valuate such services of the ecosystems, for both wild and socio-ecological production landscapes (SEPLs), and to understand the interlinkages between human, environment, and animal health. Health traditions of pre-modern societies across the globe have treated environment and human health synergistically as one health to fight many human health problems. For instance, in the Indo-Malayan realm, the Indian region in particular has an age-old non-institutional practice of local health traditions (LHTs) and maintenance of local food baskets (LFBs), with the active participation of around one million traditional healers and around 200 million informed households involving the use of over 7500 plant species (Arima & Harilal, 2018). The holistic systems of medicine that originated in India, such as Ayurveda (an alternative medicine system which postulates “Food itself is medicine and medicine itself is food”), Sidha (a traditional Tamil system of medicine), yoga, naturopathy, and Sowa-Rigpa (enriched in the Trans-Himalayan region and has similarity with Ayurvedic philosophy), put equal emphasis on the mind, body, and spirit and strive to manage health in a holistic manner. Diverse methods for improving immunity in both codified and non-codified systems and ranging from herbal water and tea, Choorna (powdered form), Lehyam (colloid form), and Kashaya (tinctures) to complex rejuvenation therapies are known in India. Plants for these preparations are often harvested from the community landscapes (SEPLs). The community landscapes are in general maintained with a mosaic of vegetation types, such as community forests, sacred groves (remnants of past evergreen forests untouched due to religious beliefs), moist bamboo brakes, bushes, scrubs, riparian forests, swamps, and marshy grasslands.
Sen and Chakraborty (2017) reported local trade of more than 1500 herbals as dietary supplements or traditional ethnic medicines in India. These therapeutic and dietary domains together produce up to 25,000 effective plant-based formulations that are commonly used by a large majority of rural and ethnic people. Although India has rich plant species with diverse folk medicinal usages recorded in the community-managed landscapes, only a fraction of these species have been studied scientifically for their pharmacological potential or health benefits.
The case reported here from the Malabar region of India is intended to throw light on the need for increasing awareness on the availability of and informed access to local medicinal and food plant diversity, healthy diets, and a favourable policy environment related to primary healthcare and production and consumption of healthy foods. The chapter points towards the need for scientific understanding of the interlinkages between the ecological heterogeneity of production landscapes, traditional resource management practices, and abundance or scarcity of plants of therapeutic, food, and health value to local communities.
2 About the International Site
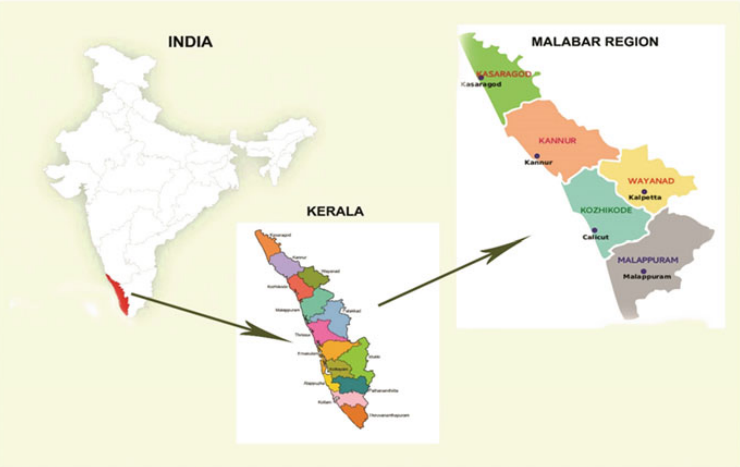
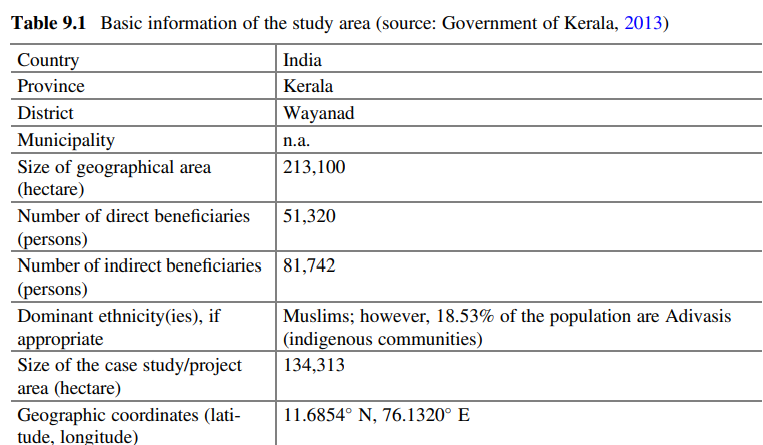
The intervention took place in the Wayanad district, a hilly terrain in the historic and globally renowned maritime destination that is the Malabar region. Wayanad terrain, covering an area of 2172 sq. km, encompasses the southwest part of the Nilgiri mountain range (7615′ –7715’E and 1115′ –1215’N). It is an east-sloping, gently undulating, medium-elevation plateau abruptly descending in the west to the Kerala plains but merging imperceptibly with the Mysore plateau to the east. Malabar is known for its rich diversity of spices like black pepper, ginger, turmeric, cardamom, and medicinal plants. For Malabar, the historic treatise of van Rheed’s “Hortus Malabaricus”, published between 1678 and 1693, is a testimony of its rich herbal heritage. Malabar is one of the richest centres of endemic, endangered biodiversity and cultural diversity of the country (Fig. 9.1). The basic information on the intervention site is provided in Table 9.1.
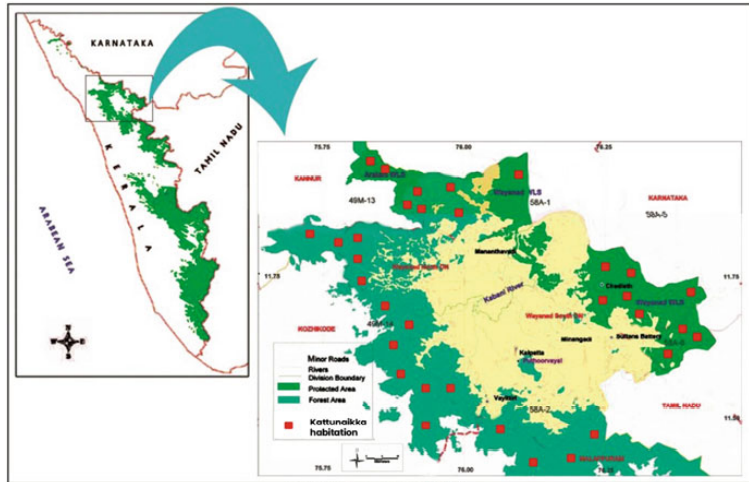
The biodiversity of Wayanad is greatly influenced by the management approaches of the diverse “sociocultural groups” that live there (Fig. 9.2). There are over 36 ethnic communities in Kerala, of which 11 are seen in the district. Farming communities in Wayanad cultivate more than 100 taxa of edible roots, tubers, and rhizomes; 20 varieties of legumes; 16 citrus cultivars; 150 vegetable varieties; and about 14 Musa cultivars (M. S. Swaminathan Research Foundation(MSSRF), 2020).
Wayanad’s population counts 817,420 people (401,684 males and 415,736 females) with a tribal population of 148,215 members, which constitutes 18.1% of the total population (Census of India, 2011).
Paniya is the largest tribal group in Kerala, and 74.49% of the population of this tribe lives in this district. The Katunaikka, a forest-dependent community belonging to the Particularly Vulnerable Tribal Group (PVTG) category, also has a wide presence. Scores on basic human development indices for education and health are alarming among both these communities. The terrain is a mosaic of diverse ecosystems ranging from mid-elevation plateau to high-range mountain landscapes with wet evergreen forests, and grasslands to dry-deciduous and scrub jungles. Apart from the wild vegetation types, the food and agricultural production landscapes are seen with certain edaphic types such as reed brakes, moist bamboo brakes, secondary evergreen forests, pseudo sholas, and marshy grasslands. Part of Wayanad’s forests is a wildlife sanctuary protected under the Nilgiri Biosphere Reserve (NBR).
3 The Intervention
The intervention of M. S. Swaminathan Research Foundation (MSSRF) in the herb-based healthcare sector among the local communities, entitled the Green Health Programme (in partnership with the Department of Biotechnology, Government of India, and a local NGO called Vanamoolika), aimed at revitalisation of primary healthcare practices and was put into action during four intermittent time periods (1998 to 2001; 2004 to 2006; 2008 to 2010; and 2015 to 2018) with the following five major activities:
- Formation and capacity-building of women’s self-help groups (SHGs) and farmers’ forums under the supervision of traditional healers, Ayurvedic physicians, botanists, and nutrition experts
- Collection, conservation, and cultivation of medicinal plants focusing on an inventory of medicinal plants known to the community and documentation of associated traditional knowledge
- Cultivation, validation, value addition, and marketing of medicinal rice called Navara (Njavara/Nakara)
- Collection, conservation, and consumption of wild food plants 5. Enriching the local food baskets by promoting home nutrition gardens
4 Key Results
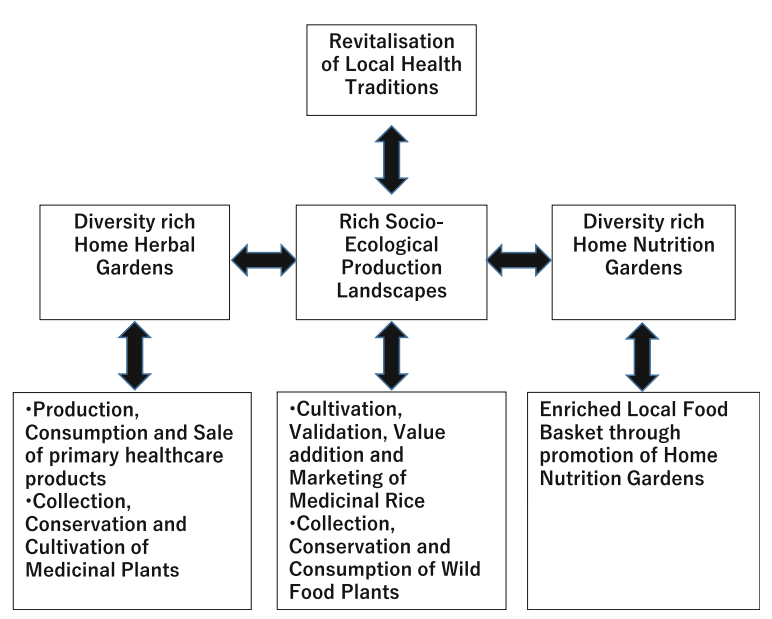
The results that emerged from the intervention revealed the SEPLs to be comprised of shade-grown coffee farms with diverse wild trees on hill slopes and integrated rice paddies in the valleys, alongside networked water canals and bushes, head ponds, and sacred groves, with many relict species still existing on hill tops and accessed by tribal and local men and women. How the interventions helped to improve human and environmental health is schematically shown in Fig. 9.3 and described herein.
4.1 Formation and Capacity-Building of Women’s Self-Help Groups (SHGs) and Farmers’ Forums
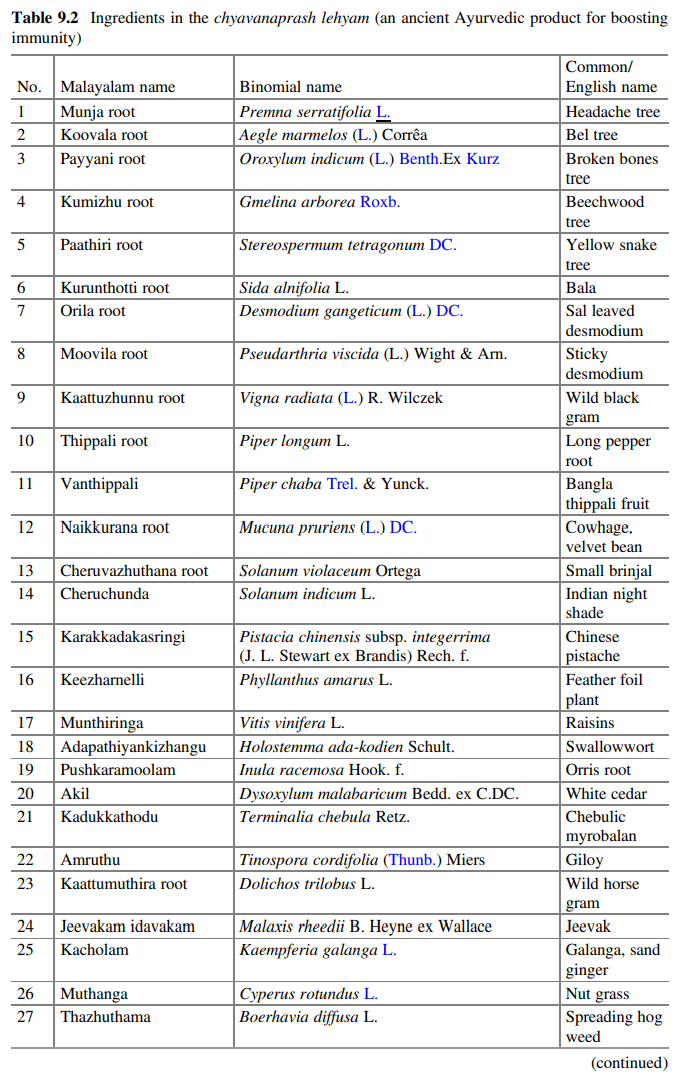
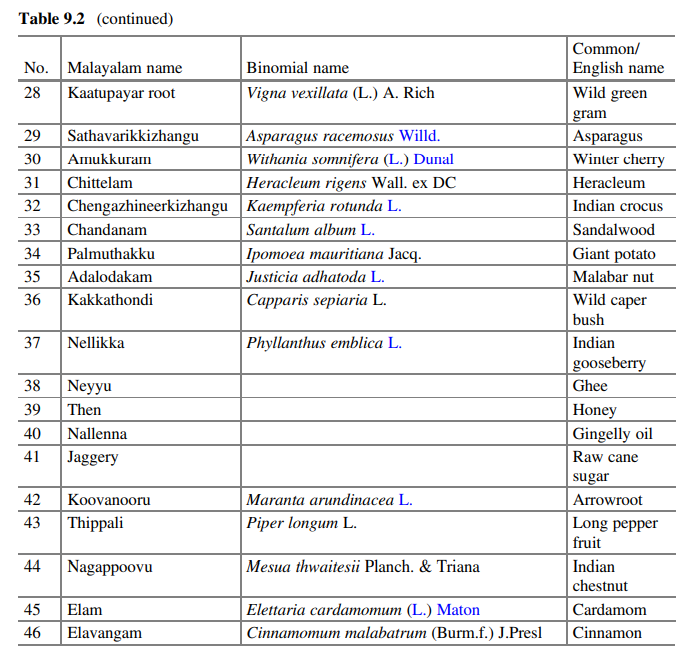
The Green Health Programme resulted in benefitting approximately 7000 rural and tribal women, including all the women SHGs and their family members and neighbours from Wayanad and the adjoining districts—Calicut and Malappuram. A total of 28 SHGs, each comprised of 10–15 women from resource-poor families, were trained, with group leaders serving as master trainers. Group members were encouraged to revitalise the practices and methods of the local healthcare systems, including medicinal plant identification, propagation, harvesting, preparation, storage, and use of primary healthcare products. Selected groups received 8 days of intensive training over a period of 8 months in the preparation of a set of 36 herbal formulations grouped into five categories: choornam (powder), lehyam (colloid form), thailam (oil), gulika (tablets), and powdered seed mixtures. One of the lehyams was “chyavanaprash”, an ancient Ayurvedic product for boosting immunity prepared using 46 different ingredients (Table 9.2). Many of the medicinal herbs needed for this preparation were once commonly available in the traditionally managed agricultural landscapes.
The concept of “People’s Biodiversity Registers” for recording of local knowledge was also shared with group members to facilitate the access and benefit-sharing mechanism. Not less than 500 awareness classes were conducted under this activity for SHG members. They were taken to observe various vegetation types, in particular the agricultural production landscapes, to help them understand the distributional differences of medicinal plants according to the land-use types. They were also allowed to visit well-reputed Ayurvedic institutions to get first-hand experience in their herbal gardens and drug production units, and to learn from their doctors.
The trained women were actively involved in the production and consumption ofseveral primary healthcare products, household-level herbal preservation, and consumption of self-prepared products made from medicinal and wild edible plants. The trainees prepared these formulations for their own healthcare needs as well as to serve as an additional income source. The quality of the new formulations was assessed before marketing with the help of well-reputed research organisations. Nine of these products that were found to have high local demand were marketed by the SHGs. Marketing was conducted through neighbourhood sales and local horticultural and seed fairs. One of the best-selling formulations, a “Navadhanya mixture” (a mixture of nine types of grains), was tested and found to be nutritionally richer than many similar products available in the market as per the results of a nutritional analysis. All groups were trained on marketing techniques and developed their own marketing strategies, with income from sales always divided proportionately among members.
The initiative began at the grassroots level and was scaled up to establish a fully equipped and licensed factory (Fig. 9.4) in Wayanad in 2008 with financial support from the state government. It is being managed by one of the partnering organisations named Vanamoolika, along with the women SHG members. Another highlight was a state government-supported project for production of ten selected herbal products. This project paved the way for organising a medicinal plant cultivators’ society named JEEVANI to help small-scale farmers cultivate and market medicinal plants. The 165 farmers registered as members in this society were linked with the Kerala Industrial Infrastructure Development Corporation (KINFRA) for large-scale cultivation of medicinal plants.
Following project activities, people who never had the habit of keeping more than ten essential species of medicinal plants started to grow many more medicinal herbs at their households. According to project records, the number of species maintained in households and nearby areas ranged from 25 to 200, and people understood their potential uses. This practice reduced the pressure on wild habitats, ensuring the sustainability and health of the ecosystem.
4.2 Collection, Conservation, and Cultivation of Medicinal Plants
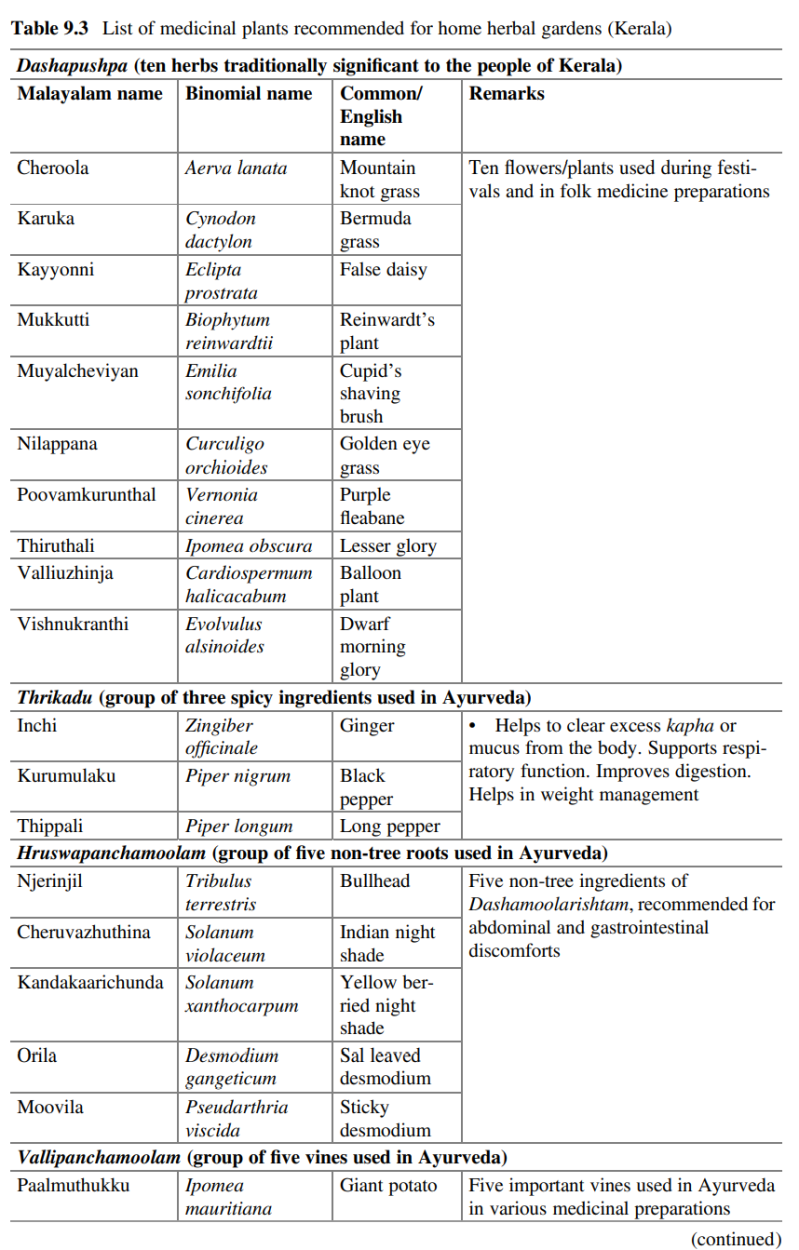
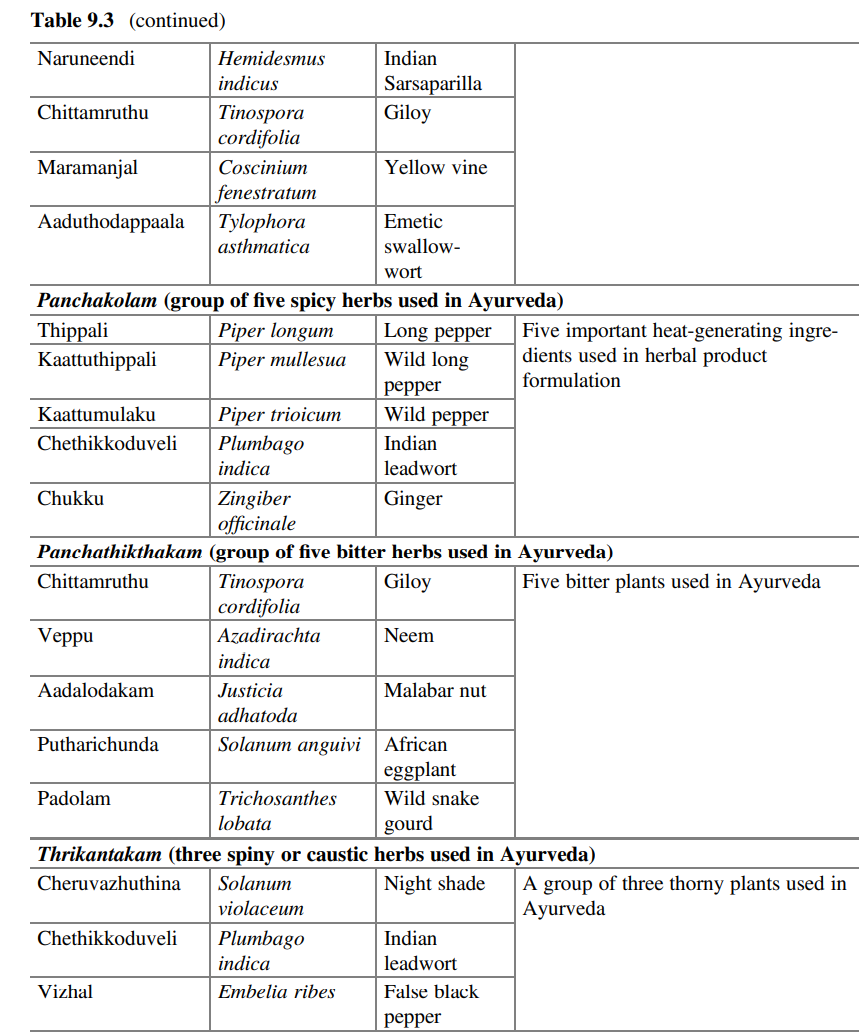
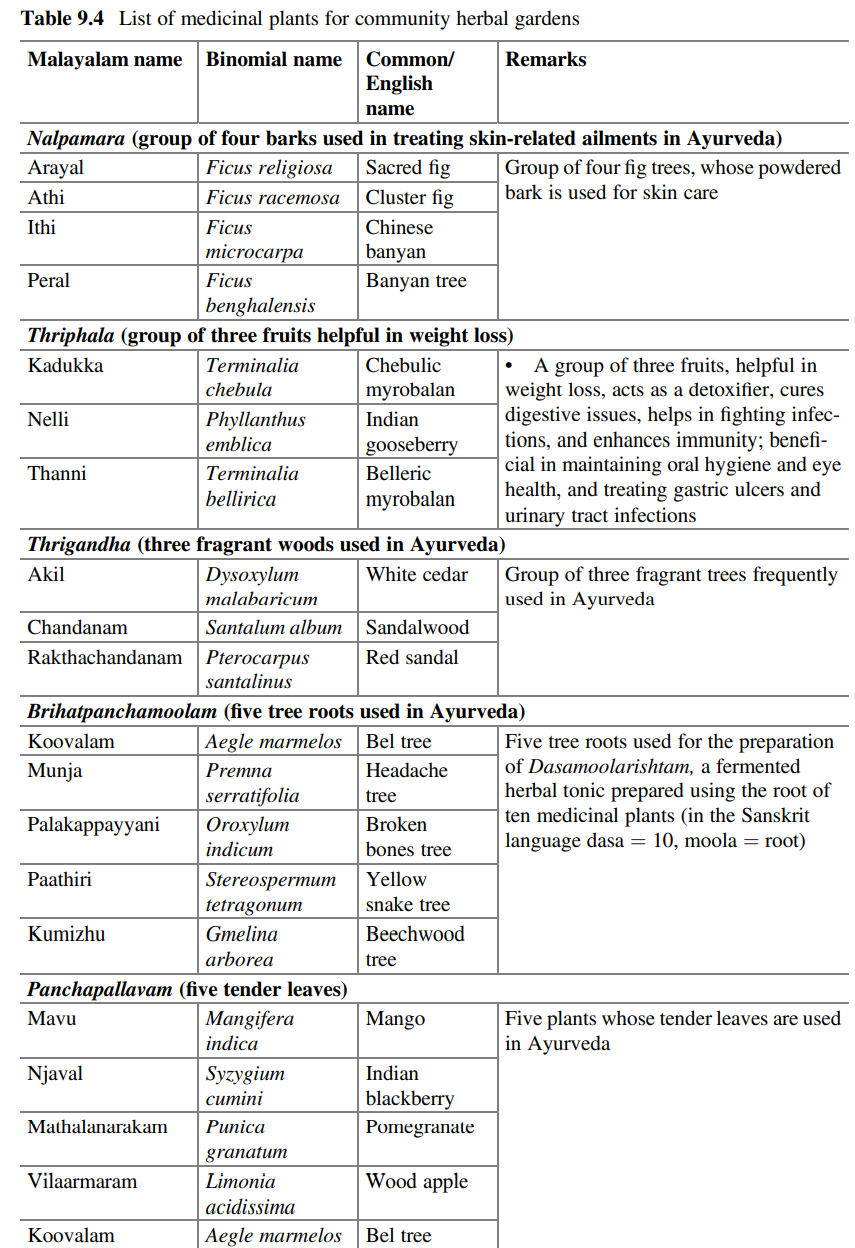
The trained SHG women also started developing herbal and edible food gardens on the premises of their homes using plants that are in high demand for making the herbal and food preparations. Herbal nurseries were set up in these gardens to raise the locally important plants that are used to prepare the 36 herbal formulations, as well as to supply identified medicinal plants to households, to promote community-level medicinal plant gardens, and for commercial cultivation (Tables 9.3 and 9.4). During the period from 2000 to 2012, the project provided seedlings of 50 species of medicinal plants important for making home remedies to 158 SHG members to set up their home herbal gardens. Also during this period, about 100,000 seedlings of medicinal plant species were raised and maintained by the SHGs in two community nurseries. The help of trained SHG members was extended to M. S. Swaminathan Research Foundation (MSSRF) to get duplicate collections of the herbal plants, which are raised sustainably by collecting only necessary seeds from wild plants, for the MSSRF’s botanical garden. One successful outcome was the conservation of superior varieties of seven selected medicinal plants: Aristolochia tagala, Celastrus paniculatus, Embelia ribes, Embelia tsjeriam-cottam, Gloriosa superba, Rauvolfia serpentina, and Saraca asoca.

4.3 Cultivation, Validation, Value Addition, and Marketing of Medicinal Rice
Navara is reported to have multiple uses. It is a nutritious, balanced, and safe food for people of all ages (Gopinath et al., 2008). The key result in this area was promotion of cultivation, validation, value addition, and market development of speciality rice varieties such as Navara and Chennellu (medicinal) and Gandhakasala and Mullanchanna (scented). The process involved collection and documentation, genetic purification (to establish distinct types of cultivars, if any), clinical validation, and biochemical analysis of Navara, and studies on value addition for the other three varieties, with a view of taking the commodities developed to non-traditional markets as a medicinal or nutraceutical package. The results were (1) cultivation of special varieties of rice in an area of 23 ha, involving 76 new farmers constituting five farmer clusters; (2) genetic purification of Navara rice at the on-farm level; (3) six value-added products developed from Navara rice put under trial marketing through a women’s initiative; and (4) characterisation of Navara golden yellow and black varieties.
The results also included reporting for the first time the occurrence of four distinct subtypes of Navara rice, which included both awned and awnless black-glumed and yellow-glumed grains (Yasmin et al., 2006). Further, more farmers were mobilised at the cluster level for Navara cultivation, and the development and promotion of a few value-added products were attempted (Kumar et al., 2003). The pilot effort to clinically evaluate the efficacy of Navara rice (yellow awnless) in collaboration with the Institute of Applied Dermatology in Kasaragod called for profiling these varieties for the presence of specific components responsible for the unique characteristics and defining of benefits for hemiplegia and other neuromuscular disorders (Guruprasad et al., 2014, p. 63). These efforts to promote high-value rice helped to check the pace of paddy field conversion to alternate crops in selected cluster areas of Wayanad, which in turn helped to enhance employment opportunities for women (Fig. 9.5, left).

4.4 Collection, Conservation, and Consumption of Wild Food Plants
A study conducted during the period 2002–2005 revealed that the tribal groups of Wayanad have extensive knowledge regarding wild food and are using a wide array of plants and animals, with variations among different tribal groups (Fig. 9.6, left). There were 372 wild edibles utilised by different tribal communities, which include 102 species of leafy greens, 19 species of Dioscorea, 40 species of mushrooms, 5 species of crabs, 39 species of fishes, and 5 types of honey (Narayanan et al., 2004; Kumar & Narayanan, 2011).
The trained tribal women of the SHGs were very interested in the wild food plants as many of the wild roots, fruits, and leaves are of high nutritional and health value to them. At one time, tribal communities had access to boundless diversity—roots and tubers, fruits and seeds, small animals that were trapped, and fish and crab that were caught, constituting a major source of their nutrition. Another result of the project was the introduction and maintenance of live collections of wild foods (Fig. 9.5, right), like Colocasia and Dioscorea tubers, in home gardens. Balakrishnan et al. (2003) reported the existence of ten species of wild Dioscorea and seven lesser known varieties in the southern part of the Western Ghats. They reported several
morphologically distinguishable species such as D. pentaphylla, D. wallichii, D. hamiltonii, and D. belophylla. Among the wild species of Dioscorea, Nallanoora (D. pentaphylla var. pentaphylla) is the most commonly consumed tuber, and D. hamiltonii and D. oppositifolia are the most frequently consumed (Fig. 9.6, right). Different tribes consume nine kinds of Dioscorea tubers, of which the most preferred are Kavalakizhangu (D. oppositifolia) and Noorakizhangu/Nallanoora (D. pentaphylla var. pentaphylla). They consider the Noorakizhangu and Kavalakizhangu to be rich in starch and fat, and the Narakizhangu (D. wallichii) to be rich in fibre.

4.5 Enriching the Local Food Baskets by Promoting Home Nutrition Gardens and Wild Food Plants
The training activities focused on the capacity-building of SHG members, Panchayath Raj Institutions (a system of rural local self-government in India elected by the local people for the management of local affairs), Anganwadi (a type of rural child care centre) workers, school teachers and students, and other community members on topics including sustainable crop cultivation practices, nutrition, agriculture-nutrition linkages, health and hygiene-related aspects, and more. Training modules included basic concept of home nutrition approach, and basic concept of a healthy and balanced diet, and culinary practices, including infant and young child feeding (IYCF) practices.
To serve as grassroots centres for nutrition intervention, nutrition gardens were established in Anganwadi centres. Community conservation plots for banana, pulses, legumes, and leafy greens were established and maintained at selected sites in the Wayanad, Thrissur, and Kannur districts. Participatory activities such as these have become even more relevant in the wake of climate change impacts on food crop species, especially in biodiversity and climate hotspots. In addition, nutritional assessment sample surveys (anthropometric and dietary) and medical camps were completed among the target groups to detect commonly existing health ailments due to nutritional deficiency.


A major result in this area was the promotion of home nutrition gardens (HNGs) for the purpose of enhancing food availability at the household level, particularly nutrient-dense foods through judicious integration of crops with animal husbandry, apiaries, fish tanks, etc. The HNG (Fig. 9.7, left and right) activities resulted in increasing (1) availability of a number of underutilised, nutrient-rich traditional and wild food crops (Fig. 9.8, left and right) and (2) availability of eggs, meat, and fish through appropriate interventions involving backyard poultry, small ruminants, and freshwater aquaculture among nearly 1000 tribal families. Also as part of home nutrition garden initiative, 30 crop varieties (pulses, roots and tubers, banana, leafy greens, and fruits) were promoted. This crop combination assures access to food almost year-round. Alongside the HNGs, efforts were taken to promote the integration of apiaries among 245 selected families scattered over the district by providing each of them with two honey boxes. The families harvested and marketed about 1200 kg of wild honey. Honey boxes placed in the vicinity of tribal hamlets helped tribal women to harvest wild honey, an activity that was earlier practised only by men. The tribal department of the state government has selected this initiative as a model for their interventions in poverty reduction in tribal areas of Kerala.
Highly motivated and progressive men and women farmers from the target villages were inducted as community resource persons (CRPs). They were skilled in various aspects of conservation, cultivation, and consumption of locale specific food crops. The pre-intervention nutritional assessment surveys helped in gathering the target groups’ food preferences in order to identify and promote suitable crops in the HNGs. Trainings were conducted targeting families on topics including crop management; maintenance of HNGs; nutritional value of crops promoted in the gardens; nutritional requirements of different genders and age groups; awareness on water, sanitation, and hygiene; and role and function of different nutrients.
Outcomes of the activities also included (1) an increased knowledge base on the region’s forest food biodiversity; (2) conservation of forest food diversity including wild relatives of some of the crops and homestead of tribal hamlets; and (3) nutritional profiling of some of the selected wild food species.
5 Discussion
Communities derive multiple benefits from SEPLs. Some of the key benefits in the case of this programme were (1) increased access to safe, traditional, and diverse foods through homestead crop diversification; (2) revitalisation of some traditional healthcare practices, which helped people to address many simple ailments on their own and in a timely fashion without rushing to the hospital or to see medical practitioners, which was otherwise common; (3) home herbal gardens with at least 25 medicinal plants at every household; (4) increased involvement in the management of medicinal and nutrition gardens; (5) increased awareness on the conservation of surrounding biodiversity; (6) considerable reduction of expenditure for food and healthcare; and (vii) additional income from sales of healthcare products.
But, despite these benefits, there has been a steady erosion of cultural knowledge, including that related to the LHTs associated with biodiversity utilisation across the targeted locations. This is mainly due to changes in the societal values and behaviours, as well as changes in the way healthcare, food production, and consumption practices are promoted by the state.
There have been a few trade-offs of the benefits community derive from SEPLs. For instance, protecting agro-biodiversity, particularly the genetic diversity of fruits and roots, from crop raiding by wild animals that are legally protected under forest and wildlife acts, is challenging. Crop raiding by monkeys, birds, wild boars, and elephants has now become more frequent in many locations that are closer to forests. Another situation is the growing trend to disband traditional joint family systems to become independent small families in order to get maximum benefits from government-sponsored schemes.
The effective management of the SEPL is mutually beneficial and could be well measured through quantitative and qualitative assessments. These measurements include changes in health and nutrition status through periodical assessments, analysis of the dietary diversity supplements provided, and intensity and frequency of health issues. For the landscape, monitoring of diversified home herbal gardens and home nutrition gardens kept enriched with plants from the wilderness, changes observed in harvesting resources from the wild, use of diverse herbal plants and wild foods that supplement the health system, regenerative agricultural fields with availability of and access to fresh water and healthy soil, and government sponsored programmes to promote tribal agriculture are some of the methods and indicators used to measure and understand effectiveness.
The SEPL in Wayanad is experiencing rapid land-use and land cover changes that negatively impact the availability of many wild species of food and medicinal value. For instance, despite the richness in the genetic diversity of medicinal and nutrient-dense rice in Wayanad that was developed and conserved mainly by local farmers, the low productivity and low profitability of these varieties alongside economic
pressures are compelling the farmers to convert the rice paddies into banana plantations. During 2006–2015, the area under rice cultivation in Wayanad drastically decreased from 21,770 ha to 8000 ha (Government of Kerala (GoK), 2015). This shift from paddy production to banana farming has had a cascading effect on the paddy wetland ecosystem. Firstly, the trend has impacted rainwater storage and aquifer recharging, and secondly, it has impacted the livelihood options of tribal communities like the Paniya, who largely depend on this ecosystem for food, employment, and income. Finally impacts have been wielded on the environment, paving the way to dump larger quantities of highly toxic pesticides for banana cultivation.
Similarly, the once species-rich shade-grown coffee farms in the region have now experienced a shift towards monocropping and high-input farming. There have been deliberate attempts to grow coffee completely exposed to sun with the high input of agrochemicals aimed at maximising crop productivity and income. This change in farming practices and intensified use of farm inputs have become major sustainability issues, particularly in the context of climate vulnerabilities. The challenges associated with climate variations result in staggering poverty, mainly nutrition and health issues, especially among the resource-poor farming communities, and the tribal communities like Paniya, Adiya, and Kattunaikka in Wayanad. Nevertheless, the growing awareness of local people on the conservation and sustainable management of SEPLs in the present scenario of food adulteration and ecosystem degradation is a green signal and opportunity to move forward.
This demands focused attention on the preservation and restoration of traditionally managed SEPLs, biocultural diversity, and revitalisation of the herbal healthcare heritage backed by scientific studies, behavioural changes, and capacity development programmes for the promotion of local biodiversity and LHTs. To address these issues, we suggest the following six integrated strategic interventions:
First, a national-level commitment to revitalise location-specific, culturally significant, and time-tested healthcare and sustainable food production practices: Integrating local health traditions and traditional medicine in the sustainable development and health agenda of the world can benefit both biodiversity and human health. A report by the WHO and CBD (Romanelli et al., 2015) discussed in detail the criticality of developing and providing cost-effective, safe, and quality-proven traditional medicine and the involvement of traditional healers in building up healthcare systems with new knowledge. Adequate investment and effective integration between different departments that deal with food and nutrition and primary healthcare promotion are required to improve human and ecosystem health.
Second, reorientation of primary healthcare services from an exogenous approach to an endogenous approach, where the focus is on the promotion of healthy foods and traditional medicine. The WHO recognises traditional medicine as an integral part of LHT, and as the “total of the knowledge, skill, and practices based on the theories, beliefs, and experiences indigenous to different cultures, whether explicable or not, used in the maintenance of health as well as in the prevention, diagnosis, improvement, or treatment of physical and mental illness” (WHO, 2013). Approaches should treat human-animal-environmental health synergistically as “One Health” to fight against any human health problems.
Third, promotion of “Green Health” practices in every home: Promotion must involve knowledgeable individuals, trained primary health practitioners, custodian farmers, tribal and rural youth, and women to focus on micronutrient-rich (naturally or chemically biofortified plants) and immunity-boosting herbals in home gardens. This can be part of promoting the concept of local health heritage villages or biodiversity heritage sites as proposed in the National Biodiversity Act (2002), wherein biodiversity is mainstreamed in the production of food, nutrition, healthcare, and livelihood needs.
Fourth, sustainable value-chain development for certified primary health-boosting foods, products, and nutraceuticals by organising a cadre of trained women’s groups in the form of herbal producer organisations: Sustainability in the supply chain occurs when management practices and governance impact positively on the socio-economic and environmental outcomes throughout the life cycles of goods and services. Sustainable commerce can be better illustrated through the 4C continuum promoted by MSSRF (M. S. Swaminathan Research Foundation (MSSRF), 2019). In this approach, commerce is done with the primary aim of creating an economic stake through options in livelihood security on small and marginal farmers, and promoted through a consumption pattern that enhances biodiverse diets, ensures food and nutrition security, and drives cultivation practices based on principles of organic farming. All of the three sector activities lead to conservation of biodiversity in situ, on-farm, and ex situ at off-farm levels. With this approach, communities can continue to engage in promoting conservation, cultivation, consumption, and local-level commercialisation of herbals, as well as plant genetic resources (PGRs) of food, nutrition, and therapeutic value.
Fifth, promotion of integrated scientific research in nutrition, health, and wellbeing to achieve health innovations and nutritional products from traditional and ethnomedicine systems through a transdisciplinary approach (by involving traditional healthcare practitioners and physicians of multiple medical sciences) to understand the bidirectional linkage between undernutrition and immunity issues and the role of nutrition and herbal remedies for a healthy life: Research in labs needs to focus on the effects of multi-micronutrients on immunity and for medical health conditions.
Sixth, restoration and preservation of SEPLs to protect from climate risks and enhance food security, water supply, and biodiversity: The buffer zones of the Wayanad district qualify as the most characteristic locations for ecosystem restoration in the Western Ghats, which itself is the highest human-populated biodiversity hotspot in the world. As 2021–2030 is the UN Decade on Ecosystem Restoration, there should be efforts from the state for a massive scale-up in the restoration efforts. This warrants a comprehensive Training of Trainers (ToT) programme in SEPLs management to offer to rural youth and officials in hill area land management, watershed development, agriculture, and allied sectors.
6 Conclusion
The COVID-19 pandemic crisis is an opportune time to seriously reflect on our indigenous traditional knowledge systems that have time-tested sustainable practices and principles in biodiversity management, and also prudence in maintaining the heterogeneity of food and agriculture production landscapes. Such practices and age-old values help local communities to keep their options alive for accessing a diverse spectrum of species of food and health value from the wild. In this context, the primary healthcare system planners need to develop a community-centric and holistic healthcare approach to effectively cater to the needs of the rural and tribal populations. The “Health for All” goal set by the United Nations in 2000 was to be achieved by adopting preventive measures, immunisation, and acquiring the capacity to access treatment and good nutrition at the individual level. Equally significant is integrating the preservation and protection of wild landscapes, ecosystems, and species diversity to succeed in this goal. This is possible if there is a transformation in the healthcare system approach by making the traditional healthcare sector as the fourth tier of the national healthcare system.
References
Arima, M., & Harilal, M. (2018). The making of local health traditions in India: Revitalisation or marginalisation? Economic and Political Weekly, 53(30), 41–50.
Balakrishnan, V., Narayanan, R. M. K., & Kumar, A. N. (2003). Ethnotaxonomy of Dioscorea among the Kattunaikka people of Wayanad District, Kerala, India. Plant Genetic Resources Newsletter, no. 135, pp 24–32, viewed 28 July 2021. Retrieved from https://www. bioversityinternational.org/fileadmin/PGR/article-issue_135-art_4-lang_fr.html
Census of India. (2011). District census handbook Wayanad, Village and Town wise Primary Census Abstract, Census of India, Trivandrum.
Government of Kerala. (2013). Panchayath level statistics 2011, Department of Economics and statistics, Kerala, viewed on 21 December 2021. Retrieved fromhttp://www.ecostat.kerala.gov. in/images/pdf/publications/Panchayat_Level_Statistics/data/2011/pswayanad2011.pdf.
Government of Kerala (GoK). (2015). Kerala economic review, State Planning Board, Government of Kerala, Thiruvananthapuram.
Gopinath, D., Singh, V., & Naidu, A. (2008). Nutrient composition and physiochemical properties of Indian medicinal rice—Njavara. Food Chemistry, 106(1), 165–171. https://doi.org/10.1016/j. foodchem.2007.05.062
Guruprasad, A. M., Saravu, N. R., Shanthakumari, V., Sushma, K. V., Kumar, A. N., & Parameswaran, P. (2014). Navarakizhi and Pinda Sweda as muscle-nourishing Ayurveda procedures in hemiplegia: Double-blind randomized comparative pilot clinical trial. The Journal of Alternative and Complementary Medicine, 20(1), 57–64.
Kumar, A. N., Gopi, G., & Balakrishnan, V. (2003). Medicinal rice of Kerala: Navara, a rice variety cultivated only in Kerala, is widely use in local healthcare systems as well as in Ayurveda for many ailments. Amruthu, FRLHT, 2, 14–16.
Kumar, A. N., & Narayanan, R. M. K. (2011). Diversity, use pattern and management of wild food plants of Western Ghats: A study from Wayanad district, viewed 12 February 2021. Retrieved from https://mssbg.mssrf.org/wp-content/uploads/2020/07/wild-food-plants-western-Ghatswebsite.pdf.
M. S. Swaminathan Research Foundation (MSSRF). (2019). From 30 years to 2030: Achieving sustainable development goals and strengthening science for climate resilience. M. S. Swaminathan Research Foundation.
M. S. Swaminathan Research Foundation (MSSRF). (2020). Draft report conservation. M. S. Swaminathan Research Foundation, Community Agrobiodiversity Center.
Narayanan, R. M. K., Swapna, M. P., & Kumar, A. N. (2004). Gender dimensions of wild food management in Wayanad, Kerala. Community Agrobiodiversity Centre & Utara Devi Resource Centre for gender and development. M. S. Swaminathan Research Foundation, MSSRF/RR/04/12.
Romanelli, C., Cooper, D., Campbell-Lendrum, D., Maiero, M., Karesh, W. B., Hunter, D., & Golden, C. D. (2015). Connecting global priorities: Biodiversity and human health: A state of knowledge review. World Health Organization and Secretariat of the Convention on Biological Diversity.
Sen, S., & Chakraborty, R. (2017). Revival, modernization and integration of Indian traditional herbal medicine in clinical practice: Importance, challenges and future. Journal of Traditional and Complementary Medicine, 7(2), 234–244.
WHO. (2013). WHO traditional medicine strategy: 2014–2023, WHO Geneva, viewed 13 October 2021. Retrieved from https://www.who.int/publications/i/item/9789241506096.
Wikimedia Commons Contributors. (2021). File:Wayanad Locator map.svg. Wikimedia Commons, the free media repository, viewed 12 February 2021. Retrieved from https://commons. wikimedia.org/w/index.php?title¼File:Wayanad_Locator_map.svg&oldid¼581468204.
{kind=link}
Yasmin, S. H., Gipson, M., Nandakumar, P. M., & Kumar, A. N. (2006). Scope of Navara cultivation. In Proceedings of the gene seminar (pp. 3–6), Community Agrobiodiversity Center.
Note
The opinions expressed in this chapter are those of the author(s) and do not necessarily reflect the views of UNU-IAS, its Board of Directors, or the countries they represent.
Open Access This chapter is licenced under the terms of the Creative Commons Attribution 3.0 IGO Licence (http://creativecommons.org/licenses/by/3.0/igo/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to UNU-IAS, provide a link to the Creative Commons licence and indicate if changes were made.
The use of the UNU-IAS name and logo, shall be subject to a separate written licence agreement between UNU-IAS and the user and is not authorised as part of this CC BY 3.0 IGO licence. Note that the link provided above includes additional terms and conditions of the licence.
The images or other third party material in this chapter are included in the chapter’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the chapter’s Creative Commons licence and your intended use is not permitted by statutory regulation, or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.